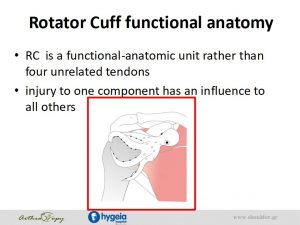
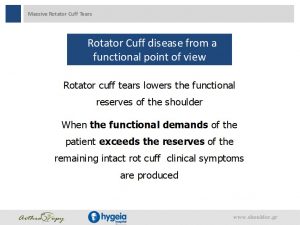
Το τενοντίου πέταλου του ώμου αποτελείται από τένοντες τεσσάρων μυών που περιβάλλουν την άρθρωση του ώμου. Οι τένοντες αυτοί προσφέρουν σταθερότητα και κινητικότητα στον ώμο.

Γράφει ο κ. Γερογιάννης Δημήτριος – Ορθοπεδικός Χειρουργός
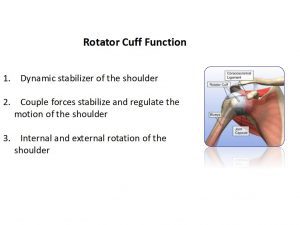
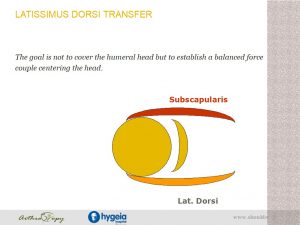
-Dynamic stabilizer of the shoulder -Couple forces stabilize and regulate the motion of the shoulder -Internal and external rotation of the shoulder












Η παραπάνω εργασία παρουσιάστηκε από τον κ. Γερογιάννη Δημήτριο στο 3rd Athens Shoulder Course